Back Pain? What to do when you throw your back out
•••••••••••••••••••••
“Throwing out your back” or acute back pain can be crippling and significantly affect your day / week. Everything seems to hurt: getting up, tying your shoes, moving, everything. What should you do? ❗️These strategies are to minimize pain and improve motion- let a medical specialist diagnose the issue.
.
Here are some methods to help you reduce your pain.
1️⃣Determine your pain triggers: it is important to determine exactly what motions cause pain. Bend forward, bend back, bend to both sides and rotate. Once you figure out what motions hurt you should avoid them. Most people with back pain have hard time figuring out what hurts. If you keep picking a scab it won’t heal. Your job is to avoid irritating the sensitive area FOR NOW. In days/weeks when your symptoms calm down you want to re-Introduce these motions.
2️⃣Gentle pain-free motion: Once you figure out what moves hurt your next job is to move in the other ways that don’t hurt. This helps de-sensitize the system and reminds your body that it can move in certain ways without pain.
?️Cat cow Exercise: on your hands and knees move your stomach up and down. Isolate movement to the spine. Complete 10 cycles of pain free motion. ?️Thoracic CARs: improve thoracic mobility to deload the lumbar spine.
3️⃣Lumbar stabilization: Pain inhibits motor activation. Therefore you want to make sure you can re-activate your lumbar musculature in a pain-free way. ?️Lumbar hinge point training: teaching the painful segment to move.
?️Positional Isometrics: at the edge of painful range of motion isometrically stabilize.
4️⃣Movement: Walking, biking, swimming. Whatever way you can without hurting do it.
Movement is medicine ✳️
✅I recommend seeing a healthcare professional. See a physician if it is required by your insurance but if you can get in quick to see a PT or chiro do it. You want to make sure this does not become a chronic issue. Back pain is the number #1 cause for disability. Even when you are out of pain I would recommend seeing someone so you have strategies to avoid this from happening again.
The oblique kick and the low side kick: How to maximally stress the knee ••••••••••••••••••••• The o
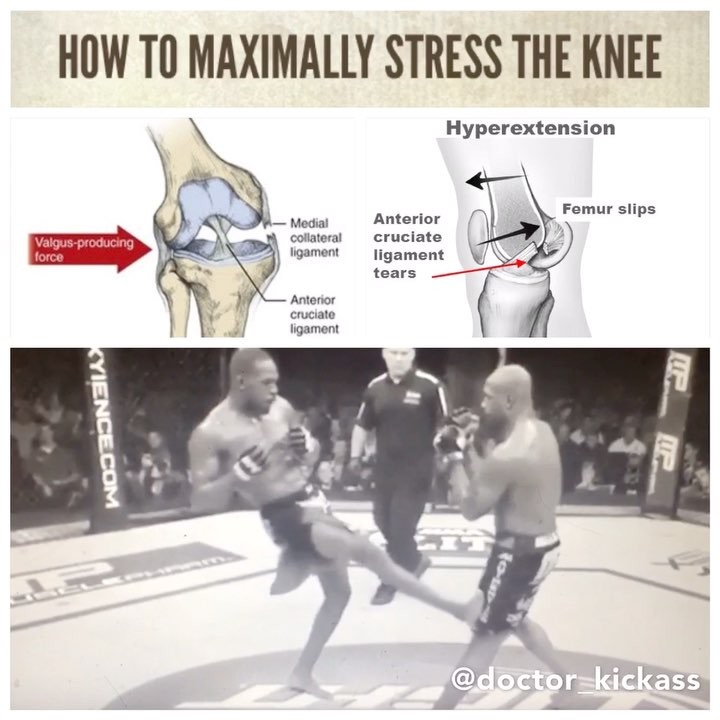
The oblique kick and the low side kick: How to maximally stress the knee
•••••••••••••••••••••
The oblique kick and low side kick are two particularly damaging strikes that are used frequently in combat sports. What makes these strike so effective? Both are effective at damaging the ligaments in the knee.
.
The goal of the oblique kick is to hyperextend the knee which can damage multiple knee ligaments.
A typical knee (tibiofemoral joint) has around 5-10 degrees of hyperextension and any more motion will challenge the soft tissue and ligamentous structures. With a trauma strike like an oblique kick one can expect:
1️⃣Muscle strain : Several muscles cross at the knee joint that can assist in resisting the motion (hamstrings, calf and popliteus)
2️⃣Ligament sprain or rupture : ACL, MCL, LCL, PCL
3️⃣Joint capsule stretch or tear
.
The low side kick often has a slightly different trajectory which may create more of a valgus force opposed to a hyperextension force. Excessive valgus on the knee isolates the MCL and ACL, however the MCL is the primary constraint against this motion. .
An example of the damage on a low side kick was @robwhittakermma vs. @yoelromeromma I. Romero threw a low side kick on Whittaker’s lead leg which was slightly sideways. Whittaker’s stance allowed the strike to create an even greater valgus force. Following the blow it was reported that Whittaker suffered a level 2 MCL sprain (major tear but not completely torn).
.
An example of the oblique kick was @jonnybones vs @rampage4real . While there was no official medical report Rampage has said that his knee was “messed up” and “had not been the same since the kick”.
.
While these kicks are considered dirty moves both of them are legal in MMA and the @ufc so it is important for fighters to be educated on the proper defense.
Kimura proof yourself: Learn how to stabilize your shoulder ••••••••••••••••••••••• Having strong an

Kimura proof yourself: Learn how to stabilize your shoulder
•••••••••••••••••••••••
Having strong and stable shoulders is crucial if you are involved in combats sports. In addition to building resilience to joint locks it is also essential for injury migration: minimizing damage for faulty falls or haphazard punches. Recently in Jiu jitsu Leandro Lo suffered a dislocation from a poor fall and in boxing Lomackenko suffered a labral tear from an aggressive lead hook. How can you strengthen your shoulders to minimize shoulder injuries?
.
Shoulder stability comes from the rotator cuff muscles. The job of these 4 muscles is to stabilize the humeral head in the glenoid fossa while the prime movers, such as the deltoids, move the arm.
.
Here are two intermediate exercises I give my patients to improve shoulder stability.
1️⃣Kettlebell bottoms up: This exercise requires stabilization of the off weighted kettlebell. Progressions to challenge stability involve adding scapular protraction (pushing shoulder blades forward) or adding a corkscrew motion.
2️⃣Kettlebell “armbar”: As someone who does jiu jitsu I hesitate to refer to an exercise as an armbar. Press the kettlebell up and rotate on your side. Maintain each position for several seconds before adjusting. This it great at challenging shoulder stability from non typical planes of motion.
.
Remember these muscles are stabilizers not prime movers so initially focus on lighter loads and high volume.
.
An important note: often when people complain about stiff shoulders it is because their joint is unstable and the muscles restrict motion. Instead of stretching a potential better alternative is to improve the stability so that the muscles can relax. Get assessed by a healthcare professional to know how to approach your shoulder.
How Leandro Lo dislocated his shoulder ••••••••••••••••••••• Leandro Lo was a favorite going into @i

How Leandro Lo dislocated his shoulder
•••••••••••••••••••••
Leandro Lo was a favorite going into @ibjjf Worlds this year to win both his weight class and the absolute however due to an unfortunate injury was unable to claim double gold. How did @leandrolojj hurt his shoulder?
.
During his final match against Mahamed Aly, Lo attempted a takedown and in the transition he had a faulty landing which resulted in an inferior shoulder dislocation. Lo was able to continue however during a sweep attempt his shoulder dislocated again and he had to concede the match.
.
The glenohumeral joint is an extremely mobile joint which means it has inherently less stability. Most commonly a shoulder dislocation occurs in an anterior position but in this case he suffered an inferior dislocation. Inferior dislocations tend to occur with impact in a hyperabducted position. Once a dislocation or subluxation (partial) occurs the static structures to assist with stability are compromised.
.
The shoulder (glenohumeral joint) involves the head of the humerus (upper arm) articulating with the glenoid fossa.
•A stable shoulder will have the humeral head centered in the glenoid fossa with arm movements.
•An unstable shoulder means the dynamic and static stabilizers are unable to keep the humeral head centered.
1️⃣Dynamic stabilizers (rotator cuff muscles): These muscles act like suction cups on the humeral head to keep it compressed and stable.
2️⃣Static Stabilizers: glenohumeral ligaments, joint capsule and labrum.
.
Hopefully Leandro Lo has a speedy recovery and can attempt the impressive feat next year.
.
References:
1️⃣Neumann, D. A. (2010). Kinesiology of the musculoskeletal system: Foundations for rehabilitation. 2. p. Mosby Elsevier.
2️⃣Wilk, K. E., Reinold, M. M., & Andrews, J. R. (2009). The athlete’s shoulder. Elsevier Health Sciences.
.
#ibjjfworlds #bjj @flograppling
Physiology of a liver strike ••••••••••••••••••••••••• In combat sports fighters often focus on aimi

Physiology of a liver strike
•••••••••••••••••••••••••
In combat sports fighters often focus on aiming for the head to finish the fight however one effective alternative is one that targets the liver. The liver is an organ that sits in the right abdominal cavity immediately behind the lowest ribs. While the ribcage does a good job of protecting many vital organs the liver remains partially uncovered and can be prone to attack. Traumatic impact to the liver, via punch, kick or knee can be excruciatingly painful and can incapacitate your opponent.
.
How can a liver strike cause this effect? .
Vasovagal syncope. The vagus nerve innervates many vital organs and connects the parasympathetic nervous system or “rest and digest” system. As the liver is one of the few organs left unprotected by the ribs when it is struck with a sufficient force it can unbalance the parasympathetic nervous system. When the system is stimulated in this manner there can be a cardioinhibitory (slows heart rate) and/or vasodepressor response (blood pressure drops). When this happens there is reduced blood flow to the brain, which can cause fainting, confusion or temporary paralysis. People often describe this feeling as their bodies turn off momentarily.
.
In boxing a liver shot is often when an orthodox fighter throws a left hook to the body against an opponent with a staggered stance. In kickboxing or muay thai this is often when a southpaw fighter throws a rear leg body kick to an opponent with a mirror stance or open stance.
.
Many strikers focus their efforts on the head but the body has many other weak points that can be exploited to win the fight.
Labral tears and combat sports •••••••••••••••••• The shoulder has the most mobil
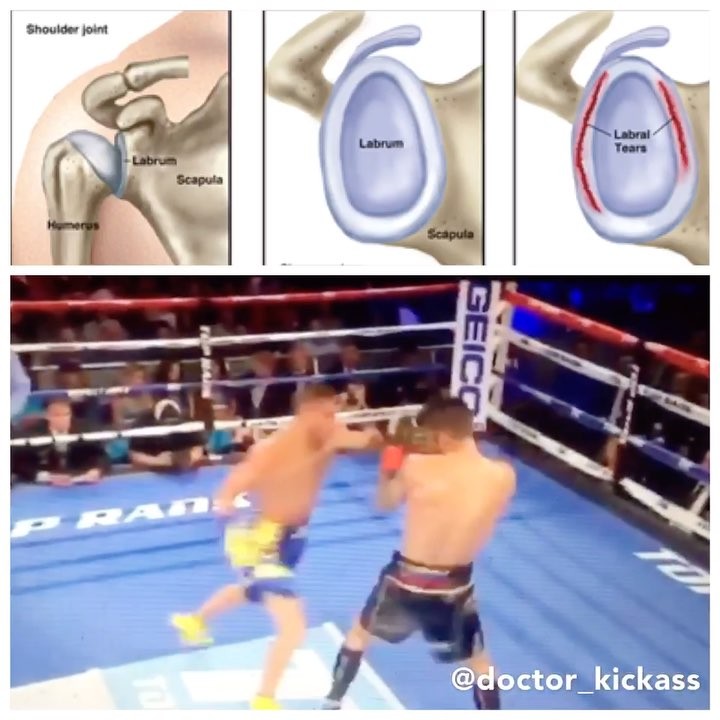
Labral tears and combat sports
••••••••••••••••••
The shoulder has the most mobility of any joint, and unfortunately the more mobility a joint has the less inherent stability there is.
.
The shoulder (glenohumeral joint) involves the head of the humerus (upper arm) articulating with the glenoid fossa.
•A stable shoulder will have the humeral head centered in the glenoid fossa with arm movements.
•An unstable shoulder means the dynamic and static stabilizers are unable to keep the humeral head centered.
1️⃣Dynamic stabilizers (rotator cuff muscles): These muscles act like suction cups on the humeral head to keep it compressed and stable.
2️⃣Static Stabilizers: ligaments, joint capsule and labrum.
Glenoid labrum: The function of the glenoid labrum is to deepen the socket for the humeral head so that it has more contact with the fossa
Shoulder dislocations: When the stabilizers fail and the humeral head translates too far from the fossa. The most common dislocation is anterior (forward). The static stabilizers often gets damaged or torn so repeated dislocations are common after the first.
Why does the labrum get damaged in fighting?
Biceps brachii is an arm muscle with two heads, and the long head of the biceps has significant attachment to the superior aspect of the labrum (up to 50%). Due to the strong connection with the labrum when there are large or repetitive forces on or from the biceps load will be transferred to the labrum. This occurs in combat sports with repetitive maximal punches.
.
An example of this was Lomachenko vs Linares. When @lomachenkovasiliy throws the lead hook it appears that his shoulder translates too far forward (anterior dislocation) and he relocates it with the excessive swing back. Following the fight it was revealed Lomachenko had a severe labrum tear and significant instability. Some labrum tears may respond to conservative treatment but in his case surgery was required.
.
References:
1️⃣Neumann, D. A. (2010). Kinesiology of the musculoskeletal system: Foundations for rehabilitation. 2. p. Mosby Elsevier.
2️⃣Wilk, K. E., Reinold, M. M., & Andrews, J. R. (2009). The athlete’s shoulder. Elsevier Health Sciences.
Falling and elbow injuries •••••••••••••••••••• The skill of falling properly is

Falling and elbow injuries
••••••••••••••••••••
The skill of falling properly is one of the most important techniques that a grappler can learn. Falling properly minimizes potential injuries to the head, neck, shoulder, elbow and wrist. Unfortunately even accomplished grapplers and fighters may land incorrectly while in the middle of a competition or fight. .
Elbow injuries usually occur when the grappler reaches out to post on an outstretched arm. The elbow often is the weakest link and the source of injury.
.
There are a variety of structures that limit hyperextension:
1️⃣muscle
2️⃣ligaments
3️⃣the bony articulation of the humerus and the ulna.
4️⃣The joint capsule is connective tissue that wraps around all three joints and is supported by ligamentous structures.
The primary ligament to limit excessive extension is the ulnar or medial collateral ligament (not to be confused with the MCL in the knee), particularly the anterior fibers which are the strongest and thickest fibers of the ligament. In addition to ligamentous support muscles of the elbow and forearm help to support and resist excessive motion, particularly the wrist flexors and pronators which act as dynamic medial stabilizers.
.
Humeroulnar hyperextension often leads to ligament strain of rupture, however if force is continued then dislocation of the ulna from the humerus can occur. While the muscles may become strained they are not likely to tear, more likely the muscle’s attachment on the ulna will rip off the main structure (avulsion fracture).
.
Continue to practice breakfalls to minimize the risk for freak elbow injuries from occurring.
The “Double Pulse”: How to generate maximum force ••••••••••••••••••••••••• In st
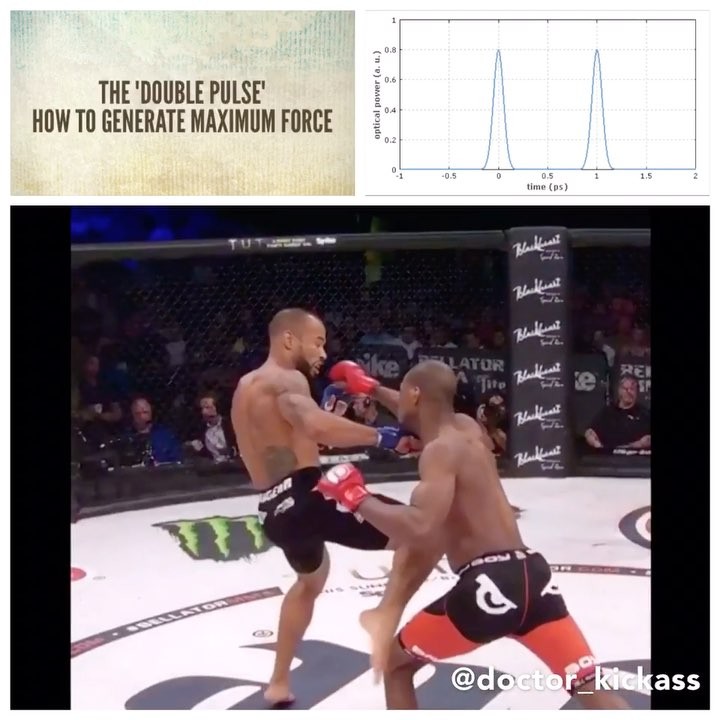
The “Double Pulse”: How to generate maximum force
•••••••••••••••••••••••••
In striking martial arts the ultimate goal is to generate power sufficient enough to render an opponent unconscious. How can one generate enough force to accomplish this task?
.
In terms of striking muscle contract to initiate the strike and create force, however a maintained contraction will slow the strike. To generate maximal force one has to contract to generate the movement and immediately relax to minimize ‘stiffness” during the follow through. Immediately before contact the contraction occurs again to create maximum force. Dr. Stu McGill refers to this as the “double pulse”.
.
McGill discovered that fighters who generate the most force are ones who have a high rate of contraction AND a high rate of relaxation. “The rate of muscle contraction, and the rate of relaxation, determines the strike speed and impact force. -Dr. Stu McGill
.
A good example of the double pulse, is @michaelvenompage ‘s knockout at @bellatormma . Page is an excellent example of a fighter who can generate power and relax at an alarmingly high rate.
.
Reference:
McGill, S.M., Chaimberg, J., Frost, D., Fenwick, C. (2010) The double peak: How elite MMA fighters develop speed and strike force. Journal of Strength and Conditioning Research. 24(2): 348-357.
How to maximally stress the MCL ••••••••••••••••••••• Here @eddie_wolverine demon

How to maximally stress the MCL
•••••••••••••••••••••
Here @eddie_wolverine demonstrates a mean sideways kneebar variation. Unlike a classic kneebar this leg lock isolates the knee ligament, medial collateral ligament. In addition to isolating the ligament there is not additional support from the bony articulation because the knee is slightly bent. This joint lock looks very similar to an orthopedic test used to assess for the integrity of the medial collateral ligament, the valgus stress test.
.
Steps to maximize the breaking force on this leg lock variation.
1️⃣ Slight bend in the knee to unlock the bony articulation of the femur and tibia.
2️⃣Externally rotate the tibia to put the MCL on stretch.
3️⃣Impart a valgus force to maximally stress the ligament. .
I would recommend caution when applying this leg lock variation to give your opponent ample time to tap before their knee ligament is ruptured.
How well does your knee rotate? ••••••••••••• As a clinician a very common findin
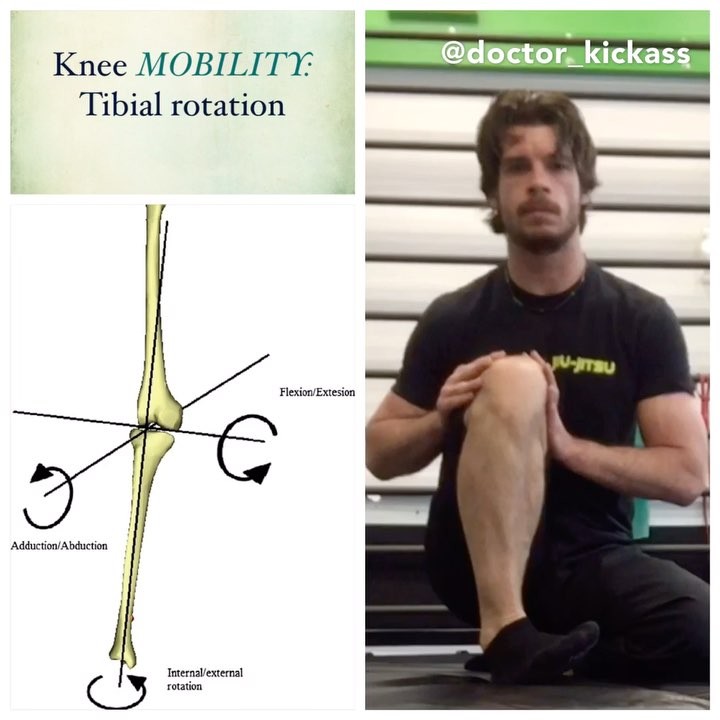
How well does your knee rotate?
•••••••••••••
As a clinician a very common finding I see is patients who are unable to actively rotate their knee (even when they are not coming to see me for a knee injury).
.
The tibiofemoral joint (knee) has 2 degree of freedom:
1️⃣bends and straightens (flexion, extension).
2️⃣shin spinning inside and outside (tibial internal and external rotation on the femur). There is a 2:1 ratio of external rotation to internal rotation, where the most rotation occurs when the knee is flexed to 90 degrees. Often clinicians focus on improving linear movement however introducing rotational movement can also improve global knee function.
.
How do you improve your ability to rotate your tibia on your femur?
•Regressed knee controlled articular rotation: Since rotation is greatest at 90 degrees of flexion this is the best place to teach someone the movement. ✅Important tip: Drive your heel into the floor and keep your toes hovering over the ground. This helps to create irradiation for maximal motor activation plus minimizes compensatory ankle movement that often creates the illusion of the tibia spinning.
.
@functionalrangeconditioning @functionalrangerelease @drandreospina @vertfit
Treating the hip capsule with functional release techniques ••••••••••••• After a

Treating the hip capsule with functional release techniques •••••••••••••
After a thorough assessment it was apparent the patient had poor hip mobility and extensibility. This was his second treatment, initially his right hip had 0 degrees of hip internal rotation.
.
Functional release treatment to the hip joint capsule:
1️⃣Anterior hip: pectineus, obturator externus
2️⃣Posterior hip: piriformis, gemelli and obturator internus.
.
The “release” mechanism involves:
1️⃣extrinsic forces: manual input with directional force on fibrotic aspects of the hip capsule.
2️⃣progressive angular isometric loading: the patient’s intrinsic isometric holds.
.
Manual treatment was followed up with FRC mobility exercises: high tension controlled articular rotations and higher tension progressive angular isometric loading / regressive angular isometric loading to lock in those improvements. .
@functionalrangerelease @functionalrangeconditioning @drmchivers @drandreospina @vertfit
Hip impingement rehab ••••••••••••••••••• Hip impingement or femoroacetabular imp
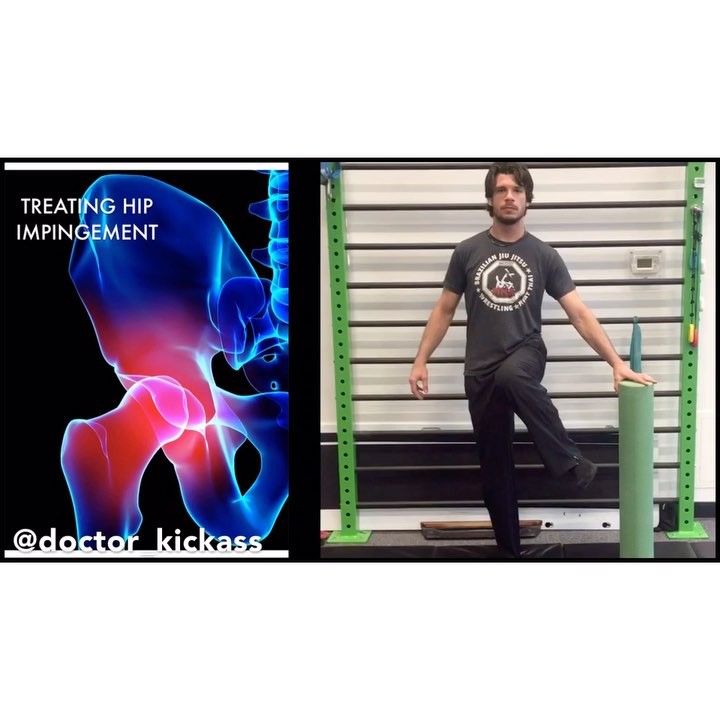
Hip impingement rehab
•••••••••••••••••••
Hip impingement or femoroacetabular impingement (FAI) is a term to describe abnormal contact with the femur and the acetabulum. If left untreated this can cause irritation and result in degenerative changes to the hip. Often this is due to anatomical variance but also this may be due to capsular tightness and poor hip motor control.
.
Impingement sign: The hallmark sign is pain with end-range flexion and internal rotation. This is a closing angle dysfunction.
.
Rehab options using FRC concepts:
1️⃣Hip 90/90 Stretch + PAIL/RAIL to reduce passive restrictions and initiate end-range motor control.
2️⃣Hip Internal rotation lift off: This is a safe position to improve hip internal rotation mobility without working in aggravating ranges of motion.
3️⃣Hip controlled articular rotations: Focus on hip rotation control.
.
Additional options may include Functional release manual techniques to the deep posterior hip capsule.
.
Those with anatomical variance may require surgical intervention but I would recommend exploring conservative treatment first.
.
@functionalrangeconditioning @functionalrangerelease @drandreospina @drmchivers @kinstretch
How to KO your opponent ••••••••••••••••••••••• When discussing striking power yo

How to KO your opponent
•••••••••••••••••••••••
When discussing striking power you have to look at several factors:
1️⃣The amount of force the athlete can generate.
2️⃣The accuracy to place that force on the optimal location. Optimal KO spots are the mandible and temple.
3️⃣The type of strike to inflict maximal damage.
.
One athlete and MMA legend who has shown exceptional ability for this is Fedor Emelianenko. While the Last Emperor may be past his prime last night he demonstrated he still has the skill to finish his adversaries very fast.
.
Throughout his career Fedor has shown an affinity for rotational strikes. In my last post I discussed the difference between linear strikes and rotational strikes.
.
“Rotational movement of the brain causes shearing forces that can lead to axonal damage. Shearing forces are most prominent near areas such as the midbrain section, where glial and axonal injury could result in severely debilitating consequences. Linear forces from a punch are often below the [mild traumatic brain injury] threshold.” This would indicate repetitive hook punches may be more damaging than jabs / crosses.
.
Model predictions have shown that the laterally impacted brain experiences a larger skull deformation, a higher in- tracranial pressure, and a higher shear deformation as compared to a brain impacted from the frontal direction. (Zhang 2004)”
.
“Higher linear and angular accelerations produced longer periods of unconsciousness (more than 3 times) on the side than at any of the other locations. (Hodgson 1983)”
.
References:
1️⃣Zhang, L., Yang, K. H., & King, A. I. (2004). A proposed injury threshold for mild traumatic brain injury. Transactions-American Society of Mechanical Engineers Journal of Biomechanical Engineering, 126(2), 226-236.
2️⃣Hodgson, V. R., Thomas, L. M., & Khalil, T. B. (1983). The role of impact location in reversible cerebral concussion (No. 831618). SAE Technical Paper.
3️⃣Safinia, C., Bershad, E. M., Clark, H. B., SantaCruz, K., Alakbarova, N., Suarez, J. I., & Divani, A. A. (2016). Chronic traumatic encephalopathy in athletes involved with high-impact sports. Journal of vascular and interventional neurology, 9(2), 34.
Training ACTIVE hip mobility •••••••••••••••••••• Mobility is the ability to acti

Training ACTIVE hip mobility
••••••••••••••••••••
Mobility is the ability to actively move ones limbs through a particular range of motion. Most people stretch to attempt to improve their mobility but this only solves part of the equation. .
“When someone wants flexibility what they really want is control.”
-Andreo Spina
.
For USABLE hip mobility one must train the tissue in a lengthened positioning (ie stretching or progressive angular isometric loading) as well as training the shortened tissue (regressive angular isometric loading). Following preparing the tissue with PAILs/RAILs one progression to improving control is by using lift offs and hovers.
.
1️⃣Lift offs are a form of mobility training that involves contracting tissue that is already in a somewhat shortened position. Some may refer to this as ‘active insufficiency’, which is the muscle not understanding how to contract any further. To improve specificity of training these are best achieved through positioning that minimizes compensatory joint motion. ?️Blocks to focus on the end-range motion.
?️Round objects positioned to minimize body leaning.
.
2️⃣Hovers are a more advanced form of mobility training focusing on controlling the desired end-range motion. Again it is best to position yourself in a manner to minimize compensatory joint motion such as leaning away.
.
Stretching is great but without an active component you will lose out on the potential benefits of real mobility.
.
@functionalrangeconditioning @functionalrangerelease @kinstretch @drandreospina